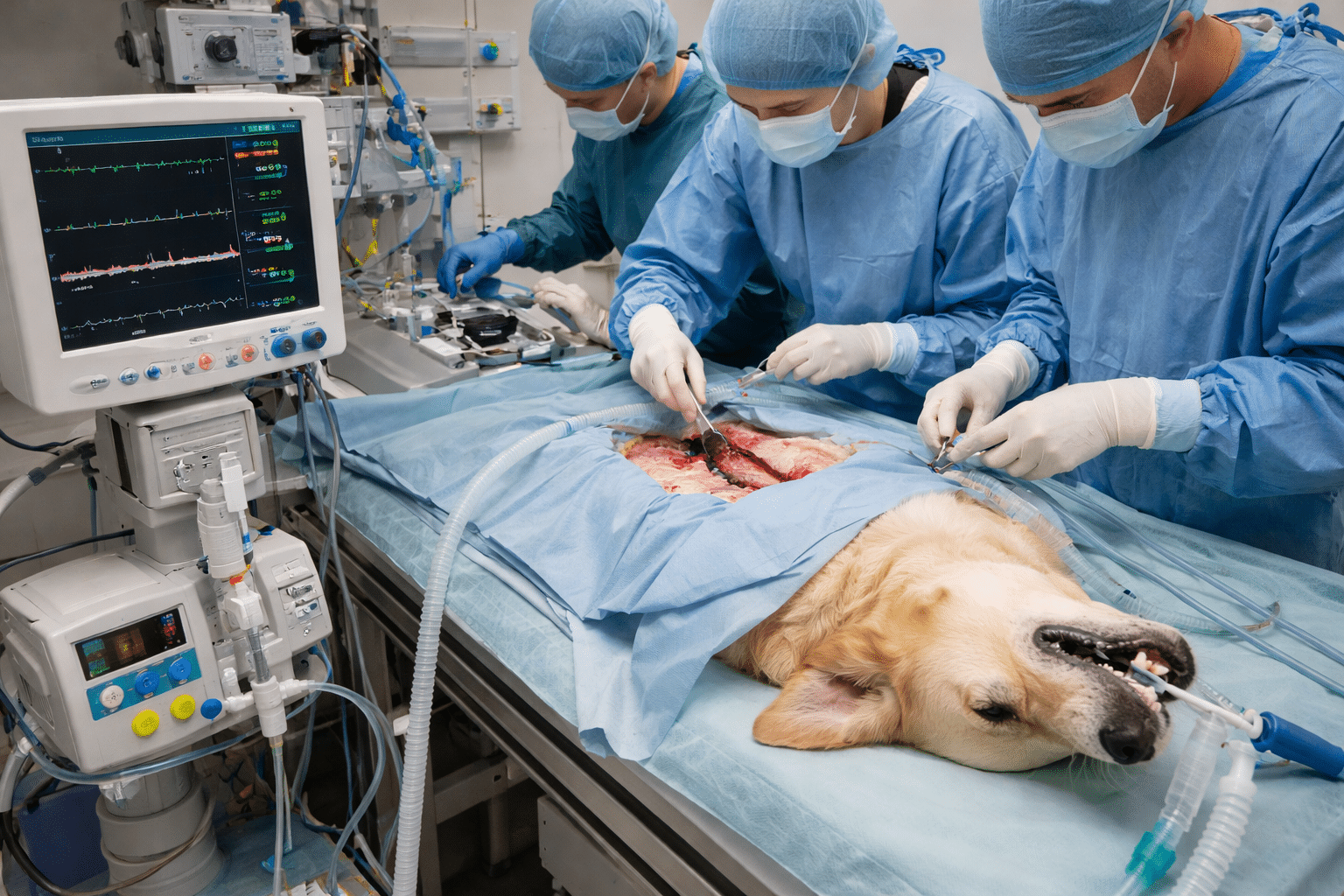
Managing Anaesthesia in Veterinary Patients with Septic Abdomen – Most veterinary emergency anesthesiologists would agree that managing anesthesia in septic abdomen patients is very challenging. Anesthetizing a patient with a septic abdomen, usually resulting from a perforated gastrointestinal (GI) tract, is one of the most difficult challenges in veterinary emergency and critical care. These patients are frequently in septic shock, in which circulation and cellular oxygenation are severely compromised. Therefore, aggressive stabilization before anesthesia is the primary objective, followed by a carefully planned anesthetic protocol with emphasis on cardiovascular stability and proper tissue perfusion.
Veterinary teams need to operate quickly, yet strategically, to stabilize the patient, limit infection, and anesthetize safely for surgical correction of the abdominal pathology.
Pre-Anesthetic Stabilization: Combating Septic Shock
Septic shock is accompanied by massive vasodilation, increased capillary permeability (“leaky vessels”), and blood flow maldistribution, which can result in severe hypotension and inadequate oxygen delivery to the tissues. Since anesthesia might cause a further depression of the cardiovascular performance, the golden rule is:
“Stabilize before you anesthetize.”
Proper stabilization can greatly enhance surgical outcomes and survival during emergency laparotomy.
Aggressive Fluid Resuscitation
Rapid fluid delivery forms the basis of treatment for critically ill veterinary patients presenting with a septic abdomen.
Setting up Vascular Access
To deliver fluids rapidly, it is crucial to have reliable access. In most cases, veterinarians insert two large-bore (18-gauge or larger) intravenous catheters, one in each cephalic vein. This facilitates the quick delivery of fluids and medications.
Which Fluid to Use
As a rule of thumb, a balanced isotonic crystalloid, e.g., Lactated Ringer’s Solution (LRS) or Plasmalyte-A, is the primary choice for resuscitation.
Fluid Administration
Instead of a big single bolus, fluids should be given in small portions. One typical approach is to administer one-fourth of the total shock volume (approximately 80-90 mL/kg in dogs) over 15 minutes and then evaluate the patient’s condition.
Resuscitation Objectives
Fluid therapy aims at effective tissue perfusion restoration. Veterinarians monitor several key parameters:
- Blood Pressure: The mean arterial pressure should be >65 mmHg.
- Heart Rate: Tachycardia should gradually improve as circulation improves.
- Lactate Levels: The level of lactic acid in the blood should decrease by 50% within 1-2 hours, which is a good prognostic indicator.
Ongoing monitoring is essential to ensure that fluid therapy increases perfusion efficiently without leading to fluid overload.
Vasopressor Therapy
Occasionally, blood pressure remains low even after large volumes of fluids have been administered. This condition is termed refractory septic shock.
Vasopressor therapy is the mainstay of treatment in these patients.
Norepinephrine is deemed the main vasopressor in septic shock as it has potent alpha-adrenergic effects that lead to peripheral vasoconstriction and result in an increase in blood pressure.
The drug is usually administered as a continuous rate infusion (CRI), and the dose is adjusted carefully until the aim of a MAP of above 65 mmHg is achieved.
Early Antibiotic Administration
Rapid response to infection is a crucial factor for saving septic patients. After the start of fluid therapy, broad-spectrum intravenous antibiotics should be administered promptly.
The most common regimen includes a combination of a beta-lactam antibiotic and a fluoroquinolone. The two drugs will cover most of the gram-positive and gram-negative bacteria associated with perforated intestines.
Early antibiotic administration helps eliminate bacteria before systemic infection progresses, and also, less inflammation will be present at the time of surgery.
Anesthetic Protocol: A Cardiovascular-Sparing Approach
When the patient has been stabilized, the anesthetic protocol can be set out. The chief purpose is to steer clear of drugs that produce major vasodilation and/or cardiac depression.
Premedication
Analgesia
A pure mu-agonist opioid is typically used for pain relief.
Fentanyl is a popular choice for the following reasons:
- Quick onset
- Short duration
- Excellent cardiovascular stability
Sedation
A benzodiazepine such as midazolam is commonly used alongside the opioid. This combination results in very effective sedation with a very limited effect on the heart function or blood pressure.
Avoid drugs such as acepromazine or dexmedetomidine because they can cause the blood vessels to relax too much and make the blood pressure drop even more.
Induction of Anaesthesia
Induction aims to use the minimum amount of anesthetic required to maintain patient stability. One commonly used method is co-induction, which involves the use of:
- Fentanyl
- Midazolam
- Gradually increased doses of ketamine or alfaxalone
Since ketamine has sympathomimetic actions, it is typically the preferred agent because it helps keep the heart rate and blood pressure at normal levels in septic patients.
Propofol should be used cautiously, as it tends to cause a very large drop in blood pressure due to dilation of the blood vessels.
Maintenance of Anaesthesia
The major challenge in maintaining anesthesia is to keep a good level of anesthesia while not compromising cardiovascular stability.
Minimize Inhalant Anesthetics
Isoflurane or sevoflurane are very potent vessel dilators. They should be used at the lowest effective concentration.
Multimodal CRI Therapy
A multimodal constant rate infusion (CRI) is the pivotal aspect of stable anesthesia.
The Fentanyl-Lidocaine-Ketamine (FLK) CRI is a very popular mixture, which provides a range of benefits:
Fentanyl: potent analgesic
Lidocaine: has anti-arrhythmic and anti-inflammatory properties
Ketamine: inhibits central sensitization and helps in lowering the amount of inhalant drugs required.
This protocol helps maintain stable anesthesia while reducing the need for inhalant drugs.
Intraoperative Cardiovascular Support
Supportive treatments should be maintained during the operation. These include:
- Continuous intravenous fluids
- Vasopressor CRIs as needed
- Constant monitoring of MAP, heart rate, and perfusion parameters
The main focus during surgery is to keep MAP above 65 mmHg.
Multimodal Analgesia
Besides ethical concerns, effective analgesia is very important physiologically. A painful stimulus increases stress response, thereby worsening shock and leading to a slower recovery.
FLK CRI
FLK infusion is the main element of intraoperative and postoperative analgesia.
Local Anaesthetic Techniques
Some further methods of improving pain control are:
- Using bupivacaine for an incisional line block before the first surgical incision
- Infiltration with local anesthetic in the muscle layers during closure
Intraperitoneal Analgesia
Apart from the above-mentioned techniques, veterinarians may perform abdominal lavage with warm saline, followed by instillation of bupivacaine before closure. This technique is very effective in managing visceral pain.
Epidural Use
Although epidural anesthesia can provide excellent analgesia, it should be administered very carefully in hemodynamically unstable septic patients, as sympathetic blockade can lead to worsening of hypotension.
Conclusion
Delivering anaesthesia to veterinary patients with a septic abdomen is a challenging task and requires quick stabilization, wise selection of drugs, and thorough monitoring. By putting cardiovascular stability first, providing aggressive fluid therapy, and multimodal analgesia, veterinary personnel can greatly enhance the chances of survival of these critically ill patients.
FAQs
Why is anesthesia risky in veterinary patients with a septic abdomen?
Anesthesia in septic patients may cause a drop in blood pressure and tissue perfusion because the tissues are poorly perfused and the cardiovascular function is depressed. Such patients are very sensitive to anesthetic drugs.
What is the most important step before anesthesia in septic patients?
The primary stabilization steps include intravenous fluids, antibiotics, and blood pressure support.
Why is ketamine commonly used in septic patients?
On one hand, ketamine has analgesic and sympathomimetic effects, which can be helpful to maintain the heart rate and blood pressure during anesthesia.
What blood pressure should be maintained during surgery?
Veterinarians typically target a mean arterial pressure (MAP) greater than 65 mmHg to ensure that the tissues receive sufficient blood.
Why is multimodal analgesia important in septic abdomen surgery?
Multimodal analgesia creates less pain, lessens the body’s response to surgery, and helps maintain stable anesthesia while reducing drug requirements.